Home Case of the Month
CASE OF THE MONTH: JULY 2019
Title: MORE THAN MEETS THE EYE
History:
This 28 years old male patient presented with chief complaints of diplopia on left lateral gaze, and restriction of left eyeball movements towards left since the past 1year. There was no history of diminution of vision on either side, sudden onset vision loss, headache, vomiting, altered sensorium, seizures, no history of facial sensory loss, or difficulty while chewing, no history of DM/HTN, or any other co-morbidity.
Examination:
The patient was moderately built, nourished. There were no neuro-cutaneous markers suggestive of any syndromic pathology. His vitals were stable. Higher Mental Function - Patient was conscious, alert and oriented. Cranial Nerves - were within normal limits except VA- right 6/6, left 6/9, left VI nerve palsy, no jaw deviation or sensory loss of the face. Motor - Bulk and Tone normal. Power is 5/5 in all groups Sensory - Touch, Pain and temperature was normal. Rest of the examination was unremarkable.
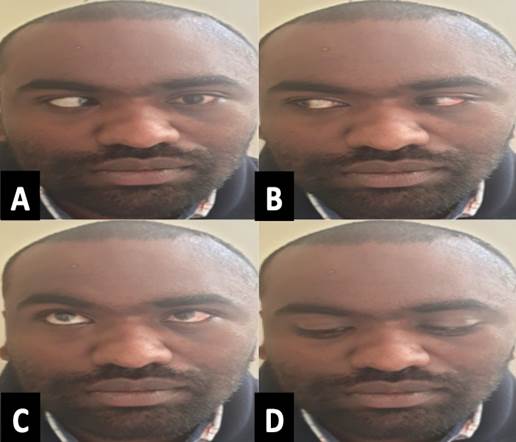
Clinical picture of the patient with VI cranial nerve palsy of the left eye
(Informed consent obtained)
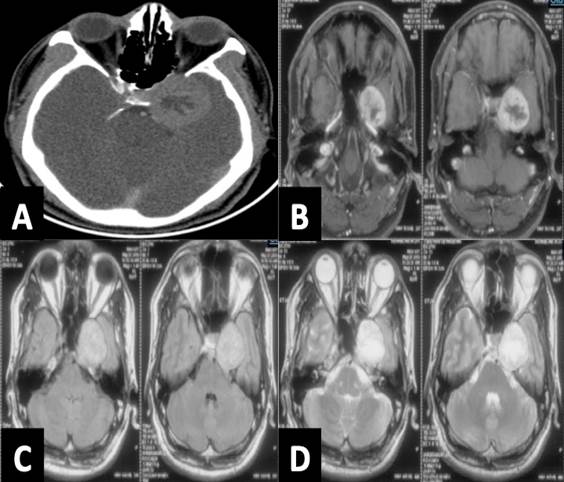
Preoperative contrast enhanced Computed tomography (a) and MRI with gadolinium contrast,T1 and T2 (b,c,d) images showing T2 hypointense-isointense lesion, T1 isointense with heterogenous contrast enhancing, at the petrous apex and medial sphenoid wing, Ipsilateral ICA is seen pushed towards right side and superiorly.
Management: The patient underwent a left fronto-temporal craniotomy and excision of lesion, lesion was completely inside cavernous sinus, and was firm, moderately vascular, Intraoperative squash/frozen section was suggestive of a schwannoma
Follow up: Patient is conscious, obeying, oriented, moving all 4 limbs, pupils 3mm BERL, left VI nerve palsy no fresh deficits.
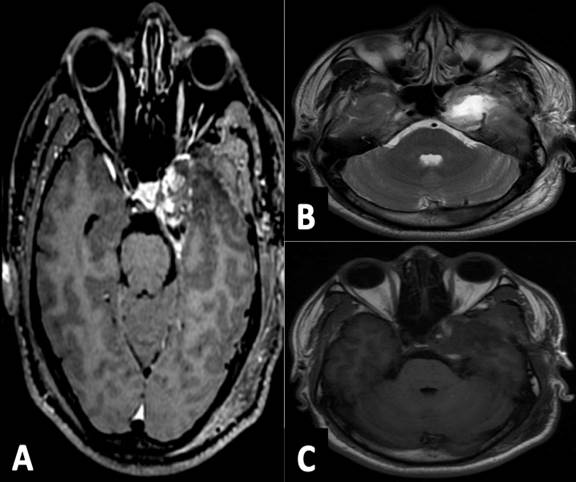
Postoperative contrast enhanced MRI with gadolinium contrast,T2 and T1 (A,B,C) images showing minimal residue in the cavernous sinus and no hematoma with temporal lobe edema
Authors: Dr. Harsh Deora, Dr. Manjul Tripathi, Dr. Abhinith Shashidhar, Dr. Malla Bhaskar Rao
Multiple Choice Questions (choose the single most suitable answer)
Question 1: Which of the following nerves has no sensory function
- III
- IV
- VI
- C and D
Submit Choice
Answer
Question 2: Which of these is not a segment of the VI nerve?
- Cisternal portion
- Cavernous sinus portion
- Orbital portion
- Sphenoidal poriton
Submit Choice
Answer
Question 3: Which of these is not a variation in the anatomy of the VI nerve:
- Variation I-70% of cases;the abducens nerve was found to be a single trunk
- Variation II-20% of cases: branching of the nerve exclusively within the cavernous sinus
- Variation III-10% of cases; duplication of the abducens nerve.
- Variation III-10% of cases; absent ipsilateral abducens nerve.
Submit Choice
Answer
Question 4: What is the incidence of post-traumatic VI nerve palsy:
- 1-3%
- 10-15%
- 5-10%
- 4-7%
Submit Choice
Answer
Question 5: Wernicke-Korsakoff syndrome has all of the following except:
- Nystagmus due to VI cranial nerve plasy
- Confusion and Confabulation
- Ipsilateral VI and VII nerve palsy
- Ataxia
Submit Choice
Answer
Question 6: What is the two types of VI nerve schwanomma except:
- Type 1: arising from the cavernous sinus leading to a sixth nerve palsy with or without mild headache.
- Type II: arising mainly in the prepontine area additionally causing signs of increased intracranial pressure.
- Type II: Arising from the nuclear level upto the caversnous sinus
- None of the above
Submit Choice
Answer
Question 7: Although olfactory nerve in itself lacks Schwann cells, the formation of schwannomas has been explained by which theory/theories:
- Developmental hypothesis which suggests transformation of mesenchymal pial cell into ectodermal Schwann cells or migration of the neural crest cells.
- Nondevelopmental theory states that these schwannomas may arise from Schwann cells of adjacent normal structures such as the perivascular nerve plexus, meningeal branches of the Vth cranial nerve, and anterior ethmoidal nerve innervating the ACF and olfactory groove.
- Both of above
- Olfactory grovve schwannomas are no such thing, only olfcatory groove meningiomas.
Submit Choice
Answer
Question 8: What are the types of III cranial nerve schwannomas except:
- Cisternal
- Cisternocavernous
- Nuclear
- Cavernous
Submit Choice
Answer
Question 9: What is the most common type of VII nerve schwannomas:
- Tympanic
- Vertical
- Labyrinthine
- Mastoid
Submit Choice
Answer
Question 10: Most common site of origin of vestibular schwannoma is?
- A.Cochlear nerve
- B. Superior vestibular nerve
- C. Inferior vestibular nerve
- D. Facial nerve
Submit Choice
Answer
Question 11: What is your level of practice:
- Resident/fellow
- Academic consultant
- Non academic consultant
- Nursing and allied staff
Submit Choice
Disclaimer